
Case 4 - Luna
Cranial Cruciate Ligament (CCL) rupture - American Bulldog, 5y, female
Luna presented with acute, severe lameness in her right pelvic limb following vigorous activity chasing a ball. On physical examination, there was localized pain and swelling at the right stifle joint.
Orthogonal radiographs revealed findings consistent with cranial cruciate ligament disease. The lateral view of the affected limb (Fig. 2) shows joint effusion along with degenerative changes suggestive of osteoarthritis affecting the distal pole of the patella, proximal trochlear groove, and fabellae. The contralateral (left) stifle (Fig. 1) appears normal and serves as a reference. A cranial drawer test was performed under sedation and yielded a positive result.
The surgical plan was developed using specialized veterinary orthopedic planning software, which allowed for precise measurements and implant selection, ensuring optimal execution of the surgical procedure (Figs. 3 and 4).
A sciatic nerve block with bupivacaine was administered as part of the analgesic protocol. Arthrotomy confirmed a complete rupture of the cranial cruciate ligament; remnants were debrided using a No. 11 scalpel blade. Both menisci were intact and stable upon probing. The caudal cruciate ligament was unremarkable. The joint was thoroughly lavaged and closed with interrupted cruciate sutures using 3-metric PDS.
Preoperative measurements indicated a tibial plateau angle (TPA) of 25°. A TPLO saw blade size 24 was used, achieving a rotation of 8.3 mm. Pre-surgical measurements were: A = 11 mm, B = 13 mm, and C = 35 mm.
A 3.5 mm TPLO locking plate was placed with two compression screws. A 2 mm anti-rotational pin was left in situ, as it did not interfere with the placement of the proximal fragment screws.
Closure was performed in multiple layers:
Pes anserinus and fascia: simple continuous pattern with 3-metric PDS
Subcuticular layer: simple continuous suture using 3-metric Monocryl
Skin: intradermal pattern with 3-metric Monocryl
Postoperative radiographs showed that the proximal screw of the distal fragment is slightly longer than expected, but this is not anticipated to cause clinical issues. GImplants are in good position, there is correct compression and alignment is also optimal.
Postoperative TPA measured at 4.3°.
Postoperative care plan:
Medications: NSAIDs for 14 days, Pardale for 5 days
Monitoring: Rechecks scheduled at 3 and 10 days post-op to assess wound healing and limb use
Follow-up imaging: Radiographic evaluation at 6 weeks
Home care: To follow printed discharge instructions form. Prevent wound licking—use a Buster collar if necessary
At the first postoperative recheck (day 3), Luna was nearly fully weight-bearing with only mild lameness. The surgical site showed excellent healing and 6 weeks post-op xrays (Figs. 7 and 8) show good ossification of osteotomy line and good position of implants.


Fig. 1
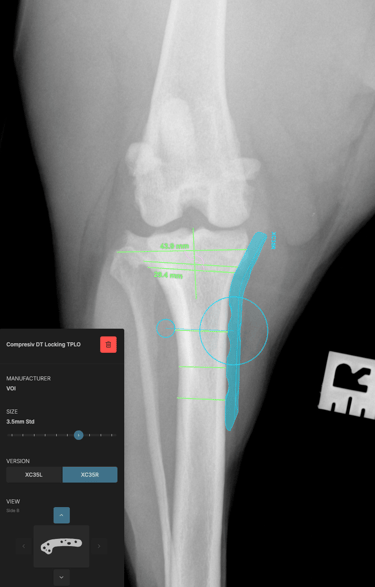
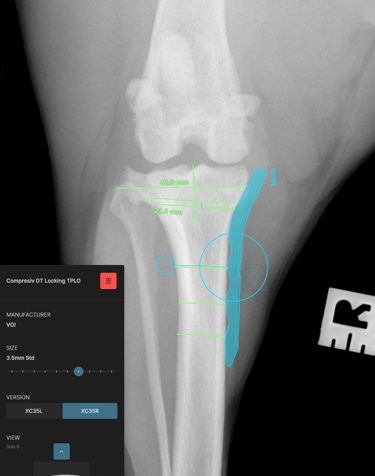
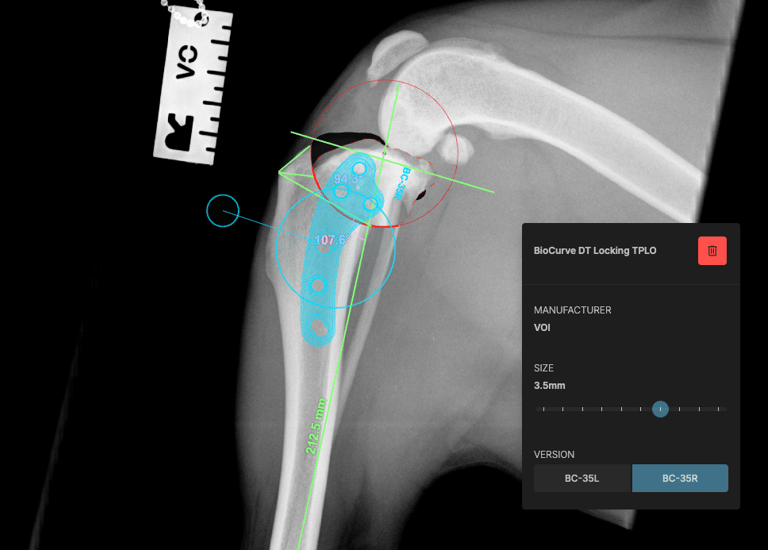
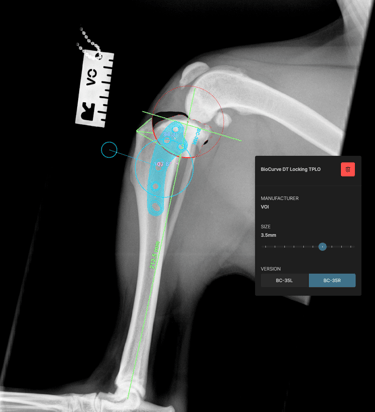
Fig. 2
Fig. 4


Fig. 3




Fig. 5
Fig. 6



Fig. 7
Fig. 8
Troya Surgery
Specialized mobile surgical services for veterinary practices.
Contact details
Email: troya.surgery@gmail.com
Telephone: 0771 625 1040
© 2024. All rights reserved.
WhatsApp: +44 771625 1040